Nullum gratuitum prandium (there is no free lunch).
Health care in America is going to cost somebody something. The question now seems to be, how much will it cost and
where are we going to find that “somebody” willing to pay. Is it really that hard to figure out what’s
wrong with our current healthcare system and come up with solutions that offer
something better than what we now have?

You can call it Obamacare, or Trumpcare, or Medicare, just
don’t call it, “I Don’t Care.” Eventually,
everybody cares. If you live long enough,
you, or someone close to you, will need something more than a Band-Aid.
Well, the first problem we have is where to find the
money. I have a few ideas that will help
us along. They may not be the total
solution, but I think most of these ideas are better than giving the wealthy deep tax cuts while shifting the healthcare burden to the remaining 99.9% of
us. Cutting taxes and cutting coverage seem
to be simple solutions developed by lazy minds. Good solutions are only difficult if you go
in trying to cut how much we spend on healthcare while looking to find ways
that private industry can make a greater profit. If you try to pair a massive tax cut for the wealthy with an improved healthcare delivery system, you are doomed. Such goals are not just unattainable they are unrealistic.
 |
| In Greed We Trust |
What would be achievable?
You could identify additional revenue sources while lowering existing
costs for healthcare. You can outline the structure for the delivery system. The one very important rule here is that everyone
must participate. Healthcare coverage
can’t be voluntary.
Why don’t we?
- Eliminate the cap on Social Security where people earning over $127,000 (in 2017) stop paying into the system. Then take the added revenue from this “new tax” and put 20% into the Social Security System and the remaining 80% into a Medicare for All Fund.
- Mandate that all employers who don’t fully provide an approved healthcare insurance plan, who have 25 or more employees and/or contractors, be required to pay $1.00 per hour into a compulsory savings plan (CSP) up to a maximum of $40 per week. Where contractors, part-time, or salaried employees can be shown to work fewer than 40 hours per week, the $1.00 per hour rate will apply. The CSP is set up for individuals and would be held in interest-bearing accounts.
- Employers who do provide an approved healthcare plan will pay a lesser amount for each employee than the amount identified in number two above. This will go a long way to make insurance “portable” in the event that employee becomes unemployed. These payments will also go into an employee identified CSP.
- Begin taxing those workers currently exempt from paying Social Security, like some federal and state employees, railroad workers, and certain religious groups. You would only tax these individuals when their salaries exceeded the current Social Security cap. For these individuals 100% of the amount collected would go to the Medicare for All Fund.
- Impose new taxes on liquor and tobacco that will go directly to the Medicare for All Fund. Charge $0.01 per ml of distilled spirits ($0.75 for a 750ml bottle), charge $0.01 per oz.) for beer (12 cents a bottle), and similar rates for other forms of alcohol. Tobacco could be billed at $0.05 per gram of tobacco in your product, which would be about $0.75 for a pack of 20 cigarettes. If marijuana is ever approved and taxed, it too would be included here.
- Raise the top marginal tax rate and raise the capital gains tax. Reagan lowered the marginal income tax rate from 70% to 28% and the capital gains tax went down to 20%. Raise both by two percentage points to help pay the cost of Medicare for All.
- Reinstate the luxury tax implemented in 1991 by George H.W. Bush but eliminated in 1993, and put it to paying for healthcare. Individuals who can afford big-ticket items like luxury cars, private aircraft, yachts, furs, and expensive jewelry can afford to help out the nation that provides them with the opportunity to make the big bucks.
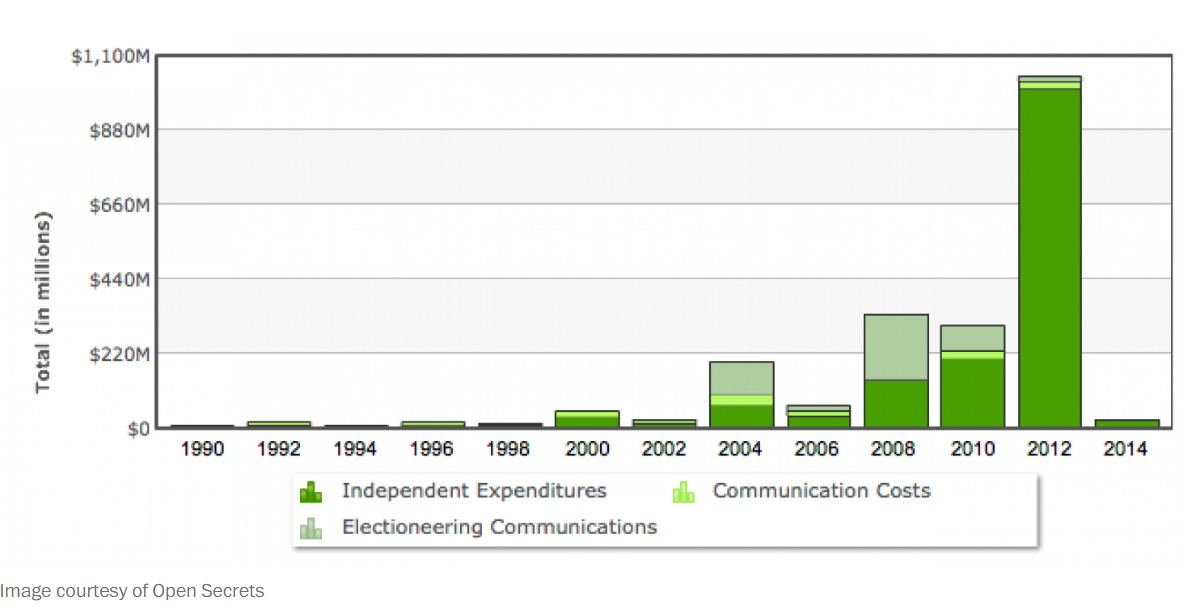
- Tax corporations and wealthy individuals who elect to make political donations to PACs and similar organizations, in excess of previously established contribution limits. They should have a portion of that donation taxed and funneled into our national healthcare coffers.
I’m sure I missed some other logical sources of revenue like
charging politicians every time they are caught in a lie, but we don’t want to
raise too much revenue. Our current
president could end up funding the entire plan.
The figures used in the enumerated points above are all arbitrary and
completely negotiable but serve as examples of reasonable sources of revenue for
healthcare.

Now, what can we do to make healthcare more affordable? Let’s reduce the cost of that care. Why not allow the Federal Government to act
as a central purchasing contractor for all medications, medical equipment, and
medical supplies. The government would
negotiate the rate that they will pay/reimburse for those items. They would be allowed to negotiate the prices
for drugs, medical supplies, and medical equipment in the global marketplace,
not just the US. Buy America first, but not exclusively at the expense of our healthcare. This one act could make
a dramatic impact on current costs.
 |
| Negotiate Prices |
All US citizens under age 65 would be provided basic Medicare
type services. The existing Medicare
structure could work where everyone is covered by the federal plan for basic healthcare. Insurance carriers could operate at the
state, regional or national levels as they choose and could offer enhanced
plans for those willing to pay. They
could use the federal negotiated rates for drugs, equipment and supplies, or
they could negotiate their own rates.
Insurance carriers would be required to offer their plans to
all residents of the states or regions where they elect to operate. National carriers would have to be open to
all citizens. The federal government
would charge a fee to all insurance carriers offering health insurance and
accordingly underwrite those carriers against catastrophic losses in the event
of pre-existing conditions or unforeseen chronic illnesses or injuries. Fees and thresholds would need to be
negotiated regularly.
No healthcare would be free.
Some form of copayment would be required for all services. Where an individual has a CSP (compulsory
savings plan), copayments would be made from that fund. There would be an opportunity, after an
individual goes on regular Medicare at age 65, to cash out any funds remaining
in their CSP, tax-free. This compulsory
savings plan would provide some incentive for people to avoid unnecessary trips
to the doctor and to try to maintain a healthy lifestyle. Stay healthy and you have money in the bank at
age 65. At $40 per week and nominal
interest, a little used CSP could have over $100,000 in it at retirement. They could then use some of this money to buy
a good supplemental health insurance plan or just take that long-postponed
vacation to Singapore.
I mentioned Singapore only because they currently have a
healthcare plan that provides better national health care coverage than the U.S. They do this for a lower per-capita cost and
provide better care. According to a year
2000 study conducted by the World Health Organization, Singapore ranks 6th
overall in the world for the quality of care.
Bloomberg ranked them as the most efficient in the world in 2014. America ranked 50th out of 55
countries in the Bloomberg review. Life
expectancy in Singapore is 82.65 while Americans can expect to make it to
78.94. While these reports, like any complex analysis, may be subject to criticism, the takeaway here is that there are many better programs in many other countries. We can and should do much better.
I don’t have access to the resources of our congress. I don't have the Congressional Budget Office to work the numbers offered here to discern their viability, but then I wasn’t elected and paid to do that job either. Come on congress. Earn your keep. You know you can come up with a good
plan. You certainly came up with a
better healthcare plan for yourselves*.

* One theory about the urgent need to repeal the ACA, put out by by Jeffery Frank of the New Yorker in his January 17, 2017 article , was that access to the Federal Employees Health Benefits Program (FEHBP) was eliminated by Article 1312 of the Affordable Care Act. The FEHBP was the wonderful plan that the Post Office, Congress, and congressional staffers had enjoyed since 1959. With the repeal of the ACA, these same government employees could go back to their original plan with all its benefits. Is Congress so devious that they would better themselves at the expense of their constituents?
 |
| I'll have what Congress is having. (scene from When Harry Met Sally) |